







This study sought to identify socio-demographic factors associated with presenting for abortion services past the gestational age limit (12 weeks), and thus not receiving services, in Mexico City’s public sector first-trimester abortion program. We found that women living in Mexico City and with higher levels of education had lower odds of presenting past the gestational age limit. Adolescents at every level of education have significantly higher probabilities of not receiving an abortion due to presenting past the gestational age limit compared with adults.
Women’s access to abortion care is often denied or hampered due to a range of barriers, many of which are rooted in abortion stigma. Abortion values clarification and attitude transformation (VCAT) workshops are conducted with abortion providers, trainers, and policymakers and other stakeholders to mitigate the effects of abortion stigma and increase provision of and access to abortion care.
This paper estimates the incidence of legal and clandestine abortions and the severity of abortion-related complications among adolescent and nonadolescent women in Ethiopia in 2014. We find no evidence that adolescents are more likely than older women to have clandestine abortions. However, the higher abortion and pregnancy rates among sexually active adolescents suggest that they face barriers in access to and use of contraceptive services. Further work is needed to address the persistence of clandestine abortions among adolescents in a context where safe and legal abortion is available.
The Youth Focused Social Network Initiative was a program to increase young women’s knowledge of and skills in accessing comprehensive abortion care in Rupandehi, Nepal from 2012-2014. The program trained peer educators to provide information and support related to comprehensive abortion care and encouraged adults to support youth in their communities. This study evaluated the effectiveness of the program and found that it had produced positive results in youth knowledge of and attitudes about comprehensive abortion care. Program expansion should be considered in light of continued need in Nepal.
The objective of this study was to determine if pregnant, literate women and female community health volunteers (FCHVs) in Nepal can accurately determine a woman’s eligibility for medical abortion using a toolkit, compared to comprehensive-abortion-care-trained providers.
Governments, advocates, providers, policymakers and other stakeholders who want to fully support women’s rights to access abortion across the globe must address quality of care, in addition to efforts to change abortion laws, train providers and expand service provision. Documenting and working to improve the quality of abortion care is necessary in order to improve service delivery and health outcomes, expand access to safe abortion especially in legally restricted settings, and to ensure the human right to the highest attainable standard of health, as outlined by the WHO.
This evaluation assesses the factors that influence contraceptive uptake among adolescents and young women seeking abortion care in health facilities. We analyzed client log book data from 921,918 abortion care cases in 4,881 health facilities in 10 countries from July 2011 through June 2015, and found that programmatic support to health systems, including provider training in contraceptive counseling and provision, was associated with women’s higher acceptance of postabortion contraception.
This study aimed to support the development of a mobile phone intervention to support postmenstrual regulation family planning use in Bangladesh. It explored what family planning information women want to receive after having a menstrual regulation procedure, whether they would like to receive this information via their mobile phone, and if so, what their preferences are for the way in which it is delivered. Participatory interviews were conducted with 24 menstrual regulation clients in Dhaka and Sylhet divisions in Bangladesh.
This paper reports the results of an intervention with 3,471 abortion providers in India, Nepal and Nigeria. Following abortion care training, providers received in-person visits and virtual contacts by a clinical and programmatic support team for a 12-month period. The intervention also included technical assistance to and upgrades in facilities where the providers worked.
Ending the silent pandemic of unsafe abortion is an urgent public-health and human-rights imperative. As with other more visible global-health issues, this scourge threatens women throughout the developing world. Every year, about 19–20 million abortions are done by individuals without the requisite skills, or in environments below minimum medical standards, or both.

Since the liberalization of Nepal’s abortion law in 2002, intensive provider training and facility support have proven successful strategies for increasing the availability of comprehensive abortion care (CAC) services in the country. However, little is known about the pathways through which women access safe abortion services. This publication presents research on how women in Nepal access safe abortion information and services, including evidence-based recommendations indicating that increasing contraceptive education and access to female community health volunteers can improve women’s ability to manage their reproductive health.

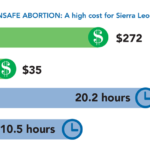
This fact sheet describes the impact of unsafe abortion in Sierra Leone as evidenced by three studies.
This guide focuses on ways to plan, implement, use and finalize an assessment of how young women and their communities relate to abortion, through locally relevant, community and/or youth-led processes. It is designed to gain insights into the local context surrounding abortion care for young women to inform program design and to support meaningful youth participation in project design. It is a global resource for community groups, youth groups, peer educators, trainers, administrators, program managers and technical advisors of abortion care programs.
Esta herramienta corta explica cómo utilizar la Escala de actitudes, creencias y acciones estigmatizantes (SABAS).
Abortion is technically legal in Zambia, but the reality is far more complicated. This study describes the process and results of galvanizing access to medical abortion where abortion has been legal for many years, but provision severely limited. It highlights the challenges and successes of scaling up abortion care using implementation science to document two years of implementation. The findings provide a case study of medical abortion introduction in Zambia and offer important lessons for expanding safe and legal abortion access in similar settings across Africa.
This analysis aimed to estimate the costs and cost- effectiveness of providing first-trimester medication abortion and manual vacuum aspiration (MVA) services to inform planning for first-trimester service provision in South Africa and similar settings. It found that the cost per complete medication abortion was lower than the cost per complete MVA. This analysis supports the scale-up of medication abortion alongside existing MVA services in South Africa. Women can be offered a choice of methods, including medication abortion with MVA as a back-up, without increasing costs.
This study looked at the socio-economic profile of women seeking abortion services in public health facilities across Madhya Pradesh state and at out of pocket cost accessing abortion services. In particular, it examined the level of access that poor women have to safe abortion services in Madhya Pradesh. Findings highlight that, overall, 57% of women who received abortion care at public health facilities were poor, followed by 21% moderate and 22% rich. Improved availability of safe abortion services at the primary level in Madhya Pradesh has helped meeting the need of safe abortion services among poor, which eventually will help reducing the maternal mortality and morbidity due to unsafe abortion.
In Bangladesh, abortion is restricted except to save the life of a woman, but menstrual regulation is allowed to induce menstruation and return to non-pregnancy after a missed period. MR services are typically provided through the Directorate General of Family Planning, while postabortion care services for incomplete abortion are provided by facilities under the Directorate General of Health Services. The bifurcated health system results in reduced quality of care, particularly for postabortion care patients. This study evaluated the success of a pilot project that aimed to integrate menstrual regulation, postabortion care and family planning services across six Directorate General of Health Services and Directorate General of Family Planning facilities by training providers on woman-centered abortion care and adding family planning services at sites offering postabortion care.