







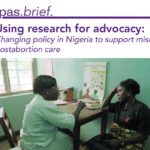
n Nigeria prior to 2009, complications from incomplete abortion were widespread and more treatment options were necessary in order to reach all women in need. Misoprostol would be a valuable addition to the treatment options in Nigeria, yet little was known about whether Nigerian women or providers would like it.
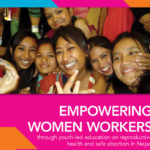
From 2011-2012, Ipas and our partners implemented a series of classes on sexual and reproductive health and rights (SRHR)—including information on safe abortion—for women who work at factories across Nepal’s Kathmandu Valley. This report explains how our project increased women workers’ knowledge of SRHR topics so they can better manage their own health and relationships and serve as resources for their families and communities. The report includes background information on Ipas’s work with youth, the context of sexual and reproductive health services for women workers in the Kathmandu Valley, details on the project’s various components, and explanation of key outcomes.
This two-page leaflet looks back at Ipas’s first forty years, pointing to our results-oriented projects and programs in more than 25 countries. It features reflections from colleagues around the world on the impact Ipas has made so far in the global movement to improve access to and delivery of safe and legal abortion care.
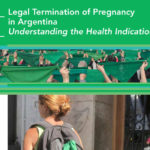
This factsheet—directed at Argentine health professionals working to improve access to safe and legal abortion—outlines a holistic approach to the application of the health indication in Argentina, in line with the World Health Organization’s definition of health and international human rights treaties.
Este documento es dirigido a las y los profesionales que trabajan por el acceso al aborto legal y seguro en Argentina. Nuestro objetivo es colaborar con la comprensión teórica y legal de la causal salud para su práctica profesional, en consonancia con los tratados internacionales de protección de los derechos humanos.
Comprehensive sexuality education (CSE) is a critical means of improving young people’s access to sexual and reproductive health (SRH) services and their ability to make safe and informed decisions. However, the topic of abortion remains absent from most CSE programs, which diminishes young people’s ability to avoid the dangers of unsafe abortion and to exercise their right to safe, legal abortion services. This factsheet summarizes the global movement to improve and expand CSE and offers key standards and approaches for creating quality CSE programs that include accurate, non-biased information about contraception and safe abortion.

Young women and girls account for nearly one-third of all unsafe abortion-related deaths each year worldwide, with 15% of all unsafe abortions taking place among adolescents ages 15-19. Despite growing global attention to the health and welfare of adolescents and girls, little is known about the abortion experiences of girls under the age of 15. This factsheet examines the unique abortion-related experiences and needs of adolescents (ages 15-19) and girls (ages 10-14), based on a comprehensive literature review Ipas conducted in 2018.

Quand il est réalisé par des prestataires formés, l’avortement est une procédure sécurisée et courante qui est autorisée par la législation de la plupart des pays pour au moins une situation. Pourtant, les femmes et les jeunes filles dans des contextes humanitaires ne peuvent souvent pas bénéficier de ce service de santé reproductive essentiel, même s’il est disponible pour le reste des femmes d’un pays accueillant des réfugiées.

In this blog (in Portuguese), Ipas senior policy and advocacy advisor Bia Galli writes that, in the wake of an historic public hearing before the Supreme Court of Brazil on the topic of abortion, it’s time to acknowledge that a democratic debate with the same diversity of arguments and plurality of views has not been possible in Brazil’s Congress. The reality and impact of Brazil’s highly restrictive abortion law continues to be ignored by parliamentarians representing religious and conservative groups opposed to reproductive autonomy for Brazilian women. In this scenario, the approval of a bill lessening restrictions on abortion is not only unlikely but utopian. Whether you are for or against the decriminalization of abortion, opposing debate on the issue is simply undemocratic.
Este juego de herramientas es un recurso para capacitadores, administradores de programas y asesores técnicos que organizan o facilitan eventos de capacitación y talleres de promoción y defensa (advocacy) en el campo de la salud sexual y reproductiva. Les proporciona a capacitadores experimentados información, materiales, instrucciones y consejos necesarios para facilitar eficazmente intervenciones de aclaración de valores y transformación de actitudes respecto al aborto.

Ce manuel est destiné à préparer les prestataires de soins à dispenser aux femmes des services de soins après avortement de qualité. Il peut être utile à un large groupe cible, notamment aux cliniciens, aux formateurs, aux directeurs de programmes et à ceux qui œuvrent en vue de l’extension des services. Il propose des informations cliniques approfondies sur les options sûres et efficaces pour une évacuation utérine au cours du premier trimestre et aborde plus largement les problèmes liés à la prestation de services et à leur accessibilité, notamment les droits des adolescentes et des très jeunes femmes, la communication entre patiente et prestataire de soins et le suivi visant à améliorer la qualité des services. Il peut être utilisé dans les pays où il n’existe pas d’indications légales à une interruption volontaire de grossesse ou dans ceux où la législation impose des restrictions importantes en matière d’interruption volontaire de grossesse.


Esta guía de referencia proporciona información y recomendaciones basadas en evidencias para el aborto con medicamentos a las 13 semanas o más de gestación, a veces denominado aborto inducido o interrupción del embarazo en el segundo trimestre, utilizando regímenes a base de misoprostol (mifepristona combinada con misoprostol, o misoprostol solo) para mujeres que necesitan un aborto inducido, tratamiento del aborto incompleto o atención postaborto. Esta guía se dirige principalmente a profesionales de la salud con experiencia proporcionando servicios de aborto de alta calidad en el primer trimestre, que desean ampliar sus habilidades para atender a mujeres a las 13 semanas o más de gestación utilizando el método de aborto con medicamentos.
Cette trousse à outils propose des ressources aux formateurs, aux responsables de programme et aux conseillers techniques qui organisent ou qui animent sur le terrain des stages de formation et des ateliers sur le plaidoyer en matière de santé sexuelle et reproductive. Elle offre aux formateurs expérimentés des informations contextuelles, des supports, des consignes et des astuces pour animer de manière efficace des interventions sur la clarification des valeurs et la transformation des attitudes.