







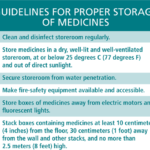

This 12-page job aid supports efficient inventory management of misoprostol (and mifepristone, depending on the setting) and other maternal-health medicines. It defines sound inventory management practices that can help reduce stock-outs and oversupply situations, and is for use by staff in public health facilities, nongovernmental organizations (civil society organizations) and private for-profit clinics and hospitals.



This is a fact sheet highlighting women’s perspectives on abortion care as part of operations research in Zambia.
Ipas works around the world every day to strengthen girls’ voices and their ability to choose the path that’s right for them.

This trainer’s manual is intended for use in training-of-trainers courses, along with its companion document, Effective training in reproductive health: Course design and delivery – Reference manual. The trainer’s manual comes with a CD-ROM that includes PowerPoint® presentations and additional exercises for the trainer.
This guide focuses on ways to plan, implement, use and finalize an assessment of how young women and their communities relate to abortion, through locally relevant, community and/or youth-led processes. It is designed to gain insights into the local context surrounding abortion care for young women to inform program design and to support meaningful youth participation in project design. It is a global resource for community groups, youth groups, peer educators, trainers, administrators, program managers and technical advisors of abortion care programs.
Sexual violence can have devastating effects on individuals, families, communities and societies. The findings from the study presented in this report are part of a regional collaboration in Central America to prevent sexual violence and to ensure that victims and survivors have access to all the services provided by the health and justice systems that they may need.


La stigmatisation de l’avortement joue un rôle central dans la marginalisation sociale, médicale et juridique des soins d’avortement à travers le monde et a des conséquences négatives sur la santé des femmes, des jeunes filles, des personnes trans et de leurs communautés. La stigmatisation de l’avortement est à l’origine du nombre élevé de décès et séquelles évitables dus à l’avortement non sécurisé à travers le monde.
Abortion stigma plays a critical role in the social, medical and legal marginalization of abortion care around the world—and it leads to negative health outcomes for women, girls, trans people and our communities. It drives the high number of preventable deaths and injuries around the world due to unsafe abortion.
Esta herramienta corta explica cómo utilizar la Escala de actitudes, creencias y acciones estigmatizantes (SABAS).
El estigma del aborto desempeña un papel fundamental en la marginación social, médica y jurídica de los servicios de aborto en todo el mundo y produce resultados negativos para la salud de las mujeres, niñas y personas trans y sus comunidades. El estigma del aborto impulsa el alto índice de muertes y lesiones evitables atribuibles al aborto inseguro a nivel mundial.
O estigma do aborto desempenha um papel crítico na marginalização social, médica e legal dos serviços de aborto em todo o mundo e leva a resultados negativos na saúde das mulheres, raparigas, transexuais, e suas comunidades. O estigma do aborto impulsiona o alto número de mortes e lesões evitáveis em todo o mundo devido a abortos inseguros.

Este juego de herramientas fue creado para proporcionar información y orientación sobre la prestación y accesibilidad de servicios de aborto inducido a mujeres jóvenes (entre 10 y 24 años de edad), según corresponda. Ofrece a capacitadores con experiencia antecedentes, materiales, instrucciones y consejos necesarios para facilitar las sesiones de capacitación de manera eficaz. Dado que los estudios de investigación realizados muestran pocas diferencias en las necesidades clínicas de las mujeres jóvenes en comparación con adultas, el juego de herramientas contiene más información sobre promoción y defensa (advocacy), alianzas y prestación de servicios que sobre temas clínicos. Es un recurso mundial para prestadores de servicios de salud, capacitadores, gerentes y asesores técnicos de programas de servicios de aborto, pero algunos materiales también se pueden utilizar para promover la participación de jóvenes, formuladores de políticas grupos comunitarios, donantes, promotores y otras partes interesadas.

Elaborados después de una investigación realizada con jóvenes en la Ciudad de México y en Tlaxcala, Atrévete a pensar diferente es una serie de tres historietas —Embarazo, Anticonceptivos, y Relaciones afectivas—que ofrecen información a jóvenes de cómo prevenir un embarazo, cómo utilizar y negociar el uso anticonceptivos y cómo mantener un relación afectiva con equidad de género. Las historietas invitan a las y los jóvenes a pensar diferente sobre su sexualidad, su salud y sus derechos.

Elaborados después de una investigación realizada con jóvenes en la Ciudad de México y en Tlaxcala, Atrévete a pensar diferente es una serie de tres historietas —Embarazo, Anticonceptivos, y Relaciones afectivas—que ofrecen información a jóvenes de cómo prevenir un embarazo, cómo utilizar y negociar el uso anticonceptivos y cómo mantener un relación afectiva con equidad de género. Las historietas invitan a las y los jóvenes a pensar diferente sobre su sexualidad, su salud y sus derechos.
Elaborados después de una investigación realizada con jóvenes en la Ciudad de México y en Tlaxcala, Atrévete a pensar diferente es una serie de tres historietas —Embarazo, Anticonceptivos, y Relaciones afectivas—que ofrecen información a jóvenes de cómo prevenir un embarazo, cómo utilizar y negociar el uso anticonceptivos y cómo mantener un relación afectiva con equidad de género. Las historietas invitan a las y los jóvenes a pensar diferente sobre su sexualidad, su salud y sus derechos.